Tympanoplasty
Surgery to reconstruct the tympanic membrane (eardrum) can be performed either under local or general anesthesia. Many patients prefer to be completely asleep. In small perforations, the operation can be easily performed under local anesthesia with intravenous sedation. An incision is made into the ear canal and the remaining eardrum is elevated away from the bony ear canal and lifted forward.
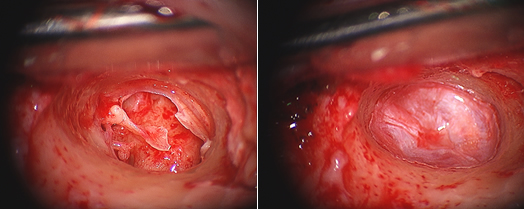
The operating microscope helps to enlarge the view of the ear structures, giving a more detailed image to the ear surgeon. If the perforation is very large or the hole is far forward and away from the view of the surgeon it may be necessary to perform an incision behind the ear. This elevates the entire outer ear forward gaining access to the perforation. Once the hole is exposed fully, the perforated remnant is rotated forward and the bones of hearing are inspected. There may be scar tissue and bands surrounding the bones of hearing. These can be removed either with micro hooks or laser.
Risks
Possible complications include failure of the graft to heal, causing recurrent eardrum perforation narrowing (stenosis) of the ear canal scarring or adhesions in the middle ear perilymph fistula and hearing loss erosion or extrusion of the prosthesis dislocation of the prosthesis and facial nerve injury. Other problems such as recurrence of cholesteatoma, may or may not result from the surgery.
Tinnitus (noises in the ear), particularly echo-type noises, may be present as a result of the perforation itself. Usually, with improvement in hearing and closure of the eardrum, the tinnitus resolves. In some cases, however, it may worsen after the operation. It is rare for the tinnitus to be permanent after surgery.